 Dr. Aristizabal's recent carrot harvest. Some of them look a little funny... Did you know that February and March are the perfect time to plant in Arizona? Many people are often surprised to learn of the many, many fruits, vegetables, and flowers that grow nearly year round in our desert soil.
What, may you ask, does gardening have to do with having babies? Gardening has so many benefits to offer pregnant women, women trying to become pregnant, and growing families. The first benefit is the simple gift of drawing us outdoors, to place our hands in the earth, feel the sun on our skin, and be aware of the sounds of birds and bees. In our highly urbanized, technical world, we need to carve out opportunities to quiet our mind and the pace of our lives. A garden demands you come outside and tend it, lest all your past efforts wilt in the dry earth. Exposure to green space has been correlated with lower levels of stress, anxiety, and depression and higher levels of emotional well-being in multiple studies, all things which are associated with higher fertility rates, better pregnancy outcomes, and happier young children. Growing fruit and vegetables also encourages us to eat more fruit and vegetables. While we should all be working to incorporate more produce into our diets, this is especially true for women who are trying to become pregnant or who are pregnant. Vegetables should make up about half of the food on our plate. Fruits and vegetables are an essential source of the many vitamins and micronutrients you need to build a healthy baby and they are much more easily absorbed from food sources than supplements. Vegetables are high in fiber, which makes you feel full without the negative effects of foods that are high in sugar and fats. When vegetables are eaten with other carbohydrates, they slow down the body’s digestion of those other carbohydrates, keeping your blood sugar more even or regulated, which not only makes you feel better, it reduces the risk of gestational diabetes and excess weight gain and decreases inflammation. Vegetables also feed healthy gut bacteria and reduce constipation. Mothers who eat diets that are low in sugar and high in produce have been shown to be less likely to deliver preterm, have children with allergies or asthma, or experience infertility. So, whether you have an acre of land or a little patio, get outside and get your hands in the dirt. It is good for you and your baby. A great resource about diet for pregnant mothers is: Real Food for Pregnancy: The science and wisdom of optimal prenatal nutrition, by Lily Nichols. If you would like to learn to garden in the desert, How to Grow your own Food, by Angela Judd, is a great resource, as is her website: https://growinginthegarden.com
0 Comments
 Well then, don’t try to have a natural birth, prepare for and do a natural birth!
It sounds like a recipe for a wild night on the beach, but no, it is just the beginning of a list of all the things people try to get labor going. Pregnant women spend the first 36 weeks of their pregnancy worrying about whether labor might come too early and spend the last four weeks (or six weeks for the unlucky) worrying that it will never come. However, it is not so easy to understand what might actually bring about labor too soon or help it along when a pregnancy extends past its expiration date or a mother’s (or her doctor’s) tolerance. There is a nice little analogy I came up with a few years ago to help my patients understand this complicated process. It starts with a horse in a barn, because, well, I am from the southwest and we talk about things like horses and barns. The baby is the horse:  The horse lives in a barn:  Around that barn, is a fence: 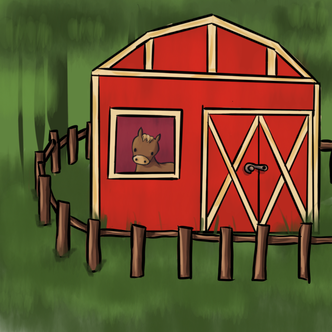 And all the other little horses, or babies, are out in the pasture:  The horse lives happily inside your uterus until, eventually, usually between 37 and 41 weeks after conception, it decides it wants to get out, but it doesn’t just want out of the barn, it wants past the fence and out to pasture with all the other baby horses. The horse, your baby, is the one that decides to get out of the barn, and sends that signal for labor to start. So why do people even bother with things like sex, pineapple, acupuncture, evening primrose and all the other things people try to get into labor, or why do they tell women to avoid sex if there is a concern about premature labor? If the horse is the one that decides to get out of the barn, how do any of these things work?
However, if our barn door is functional and locked up tight, we can leave our fence gate as open as we like, and that little horse is not going anywhere.   One of the most commonly repeated “alternative facts” in the natural birth community is that women in labor are aided in the process by gravity and, thus, should be encouraged to labor and push in upright positions. Pregnant mothers will come across this in nearly every natural labor text, website, or blog and, on the surface, it seems to make a lot of sense. Why not let the force of gravity work for you? Why work any harder than you have to?
This gravity idea causes a lot of anxiety in pregnant mothers and they often fear that they will be “tied to the bed” or have to deliver “flat on their backs,” working against gravity. I will often be working with an exhausted mother, who is pushing well on her back and has no energy for any other position, that suddenly cries out, “but shouldn’t I try to get up so I can get some gravity?” But the simple fact is that gravity has nothing to do with getting a baby out. If it did, babies would be falling out of women left and right and there would be little need for advice about birth. No, getting a baby out is about moving a baby past an obstruction: the mother’s cervix, soft tissue, including cartilage and muscle, and the hard bones of the pelvis. In order for this to happen, the mother’s soft tissues need to mold, stretch, and relax and the connections between the bones in the pelvis need to loosen. Adequate force must then consistently work the baby through these structures. The baby has to rotate into different orientations so that it may move more easily through pelvis and the bones in the baby’s skull must shift and mold in order to decrease the diameter of the baby’s head squeezing through this narrow passage. It is an extremely complicated process and given that mothers and babies come in all different shapes and sizes, it is no wonder that it can be a significant challenge to achieve. This is not to say that freedom of movement, ambulation, and alternative pushing positions do not benefit women in labor. They do. Studies have shown that mothers who are able to move freely throughout their labors report less pain, have shorter labors, and less need for pitocin and epidurals. Alternative pushing positions, such as hands-and-knees, side lying, and squatting, are associated with less perineal tearing, shorter pushing stages, and less observed fetal heart rate changes, however in the studies that have been performed, no one pushing position was so superior as to consider it a preferred position for delivery. Furthermore, none of the studies examining position in labor and specifically pushing positions have demonstrated higher spontaneous vaginal delivery rates in mom’s who spend their labors upright or push in upright positions. In fact, a recent well-done study in the UK which specifically looked at women with epidurals, found that women who pushed on their backs actually had higher vaginal delivery rates than those that sat upright, even though their deliveries where performed by midwives who reported that they believed upright positions were superior. (Upright versus lying down position in second stage of labour in nulliparous women with low dose epidural: BUMPES randomised controlled trial. BMJ 2017; 359 :j4471) The apparent conflict in these observations is because the forces acting on a baby during labor and causing changes in the mother’s body are internal, not external. The observed benefits of alternative positioning are not due to the external force of gravity, but are due to their direct effect on the mother’s musculoskeletal system, which alters the dimensions of the maternal pelvis and the direction in which internal forces are acting on the baby. The combination of these factors aid in rotation and proper alignment of the baby’s head with it’s mother’s pelvis. Anything that enables proper muscle relaxation and alignment of the fetal head in the pelvis can achieve this same effect, including hydrotherapy or even an epidural. Any position that allows the forces of uterine contractions and maternal pushing to effectively move a baby through the pelvis is a good position. For some women that will be upright, for some women that will be a side-lying position, and for others it will be on their back. So, long story short, a laboring mother should be encouraged to try many different positions during labor and delivery, in order to help her relax, labor in the way most comfortable for her, and move her baby through her pelvis effectively. If something doesn’t seem to be working or doesn’t feel right, she should simply try something else. There is no right position for every woman or every baby or even one single labor and there are times that lying down may be just what a woman needs.  In the natural labor world, there are tales of a mystical, magical creature: the Unicorn Birther. The Unicorn Birther is a woman who somehow reaches near complete dilation with little to no discomfort and only mild, infrequent contractions. Many people confuse the Unicorn Birther with women who manage their labors extremely well, utilizing breathing and other techniques. I commonly see patients who have studied Hypnobirthing who resemble Unicorn Birthers in their calm demeanor, but a true Unicorn Birther is something very different. Women who cope well with labor will still communicate discomfort and have contractions in short intervals that build both in intensity and frequency as the labor progresses, while Unicorn Birthers will look at you, smiling and bewildered when asked about discomfort, reporting only a little tightening or pressure. The other type of woman who is often confused with a Unicorn Birther is the woman who has a very fast labor, what is referred to in the medical community as a precipitous birth. However, anyone who has taken care of a woman delivering precipitously or anyone who has had such a labor can tell you that it is far from a serene experience. This labors are usually fast and furious, with strong, frequent, and painful contractions that seemingly come out of nowhere and result in a bright red, mad and screaming infant in under four hours. This is very different than a unicorn labor.
It has been estimated that as many as 1% of women fall into this category, reporting little to no pain in labor, but it is still a fascinating experience to work with the real life, walking and talking version of these tales, even when you have seen it before. Just recently, I helped a Unicorn Birther deliver her baby, staring at her in disbelief, as she bounced around the labor room, contracting only every six or seven minutes, smiling, laughing, with perfect makeup and beautiful eyelashes at a good eight centimeters of cervical dilation. I would watch each contraction peak on the monitor, but her smile was unmoved. Sometimes she would touch her belly, feeling the firmness, and state that she “thought” that one may have been stronger. I found myself surprised and relieved that she was aware enough of her body to come to the hospital rather than having her baby on the kitchen floor. However, very interestingly, of all the Unicorn Birthers I have delivered, I have never had a single “easy” unicorn delivery. Each one of my unicorns have, in fact, had a malpositioned, usually sunny-side up or OP, baby that did not descend into the pelvis without a whole lot of encouragement. This may be why the sensations of labor are so different for these patients, the lack of decent with a cervix that somehow dilates nicely despite the baby remaining high in the pelvis. In each of my experiences with unicorns, once their babies finally did descend, typical sensations of labor ensued and suddenly they looked like normal laboring women, though they often delivered so quickly that the story remained that the labor was essentially pain free. So, what can these Unicorn Birthers teach us mere mortals about pain in childbirth? Probably something we already intuitively know: that much of the pain of childbirth comes from the forces of labor moving the baby against resistance: the resistance of the not yet fully dilated cervix, the resistance of the muscles, soft tissue, and bones of the pelvis, and finally the resistance of the vaginal wall. When we lessen the resistance, the pain of labor is reduced. This is why epidurals contain medicine to relax the mother’s muscles, not just numb pain sensations. This is why labor tubs relieve pain, the buoyancy lessens the effective weight of the baby moving through the pelvis, thereby reducing the friction acting against it. This is also why mothers who have labored previously often do not feel painful contractions until much later in labor process, as their tissues and pelvis are already stretched and do not resist the descent of the baby to the same degree. This is why meditative methods of childbirth are the most effective. Women learn to control their responses to discomfort and relax their bodies, allowing their labors to progress in an easier fashion. It is also why alternative positioning that promotes an open and relaxed pelvis is usually more comfortable and effective than more constricted positions. Ultimately, birth is something you must flow with, not fight against  Many of my scheduled appointments each week are what we call in our office a “preconception consult.” This is a visit where a patient is planning a pregnancy and wants to get to know our practice, make sure they are healthy before getting pregnant, and receive information or help with conceiving. There are also a certain percentage of these visits that are what I call “the VBAC interview.” These are patients who had a previous cesarean and are trying to find someone who will “let” them have a vaginal delivery in a future pregnancy. They will often dance around the questions they really want to ask, trying to figure me out and whether I am really VBAC (Vaginal Birth After Cesarean) friendly. I try to quickly relieve them of this anxiety and cut to the chase: “I see you had a previous cesarean, where you hoping for a vaginal delivery with this upcoming pregnancy?”
Unfortunately, more and more women are finding themselves in the position of having to explore their options after a previous cesarean. According to the CDC, 21.8% of women, 1 in 5 women, who have never had a cesarean before, will deliver via cesarean. If these women go on to have another child and desire a vaginal delivery, their chances of actually delivering that way are small. Only 12.4% of women with a previous cesarean will have a VBAC in a future delivery, despite the fact that a VBAC can be successful over 80% of the time it is actually attempted. While there are certainly patients who make an independent decision to have a repeat cesarean, there are many more who want a VBAC who are not being given the chance. As an obstetrician with a large percentage of patients who choose me specifically for a VBAC, I have an insiders take on what it really means to be a VBAC-supportive provider and how women can identify whether or not they have one. Here are the four most important questions women who desire a VBAC should be asking:
There are certainly many other questions that can signal incomplete VBAC support, but these questions get to the heart of VBAC support and can quickly help a woman decide if her current care provider will really help her reach her goal of a vaginal delivery. For help in finding a VBAC-friendly practice, reach out to your local ICAN chapter  I was recently giving a presentation regarding natural birth and low intervention models of care to a group of physicians at one of my local hospitals, which coincidentally has one of the highest cesarean rates in the country. I am accustomed to receiving push-back regarding my support of natural birth from members of the medical community, just as many women seeking a natural birth receive push- back from their providers. However, one of the comments at the end of my presentation struck me, particularly because I did not have the chance to respond, as his comment dragged past our time limit and he claimed the last word. The commentator was obviously very disturbed by my argument that women should have autonomy over their birth process and a right to share in the decision making with their care provider. He insisted that obstetricians were like pilots on a plane. No one questions the pilot’s decisions regarding how to safely get a plane from point A to point B and, likewise, patients should not be questioning their doctor’s judgement, given their years of training and expertise, to safely care for them during labor and delivery.
Many in the room agreed with him and at first blush, it is a convincing argument. Of course, any surgeon provides care that is comparable in the skill level to that of other highly specialized professions, such as pilots. Certainly, when the time comes to actually perform the procedures needed by their patients, such as a cesarean or vaginal delivery, women must trust that the training and credentialing of their physician is sufficient to enable them to safely perform that procedure, as we trust when we sit down in our plane seat that the pilot on board has the proper training, credentials, and oversight to carry us to our destination in one piece. Women are not asking to fly the plane. They simply want to be able get up and move around during the flight, except during the higher risk times of takeoff, landing, or turbulence. But, if that fasten seat-belt sign is left on too long or activated too often, the passengers may begin to question whether it is truly necessary and a brave few might even begin to roam the isles. They want to be seated with their travel companions and have enough space to relax. They want to be able to turn off their passenger light and have a quiet environment to travel in. They want comfort and care from their flight attendant. They want to eat and drink, even if there is a chance they might get a little nauseous while on board. They want to be able to pick their flight and they don’t want to be forced to take a sedative before getting on board. They also want guidelines and check-off's in place to promote safe, uneventful flights with very little use of the pilot’s many highly specialized skills. The pilot shouldn't fly the plane too fast just because they believe it is more efficient or they want to go home. The vast majority of the time, the flight should be on autopilot. While a pilot may be skilled enough to perform a crash landing, if he or she was doing that on any regular basis, it would not be considered a good thing. It is okay to question the judgement of a system that is landing at the wrong airport 32% of the time, which is the national rate of cesarean, and crash landing far too often, with frequent near misses in maternity care. It is okay to say that level of restriction on ambulation, diet, time in labor, and access to alternative comfort strategies is not necessary for patient safety. It is okay for women to have a say about their flight experience.  There is no shortage of natural birth books. I should know. My bookshelves are full of them and, as an obstetrician who cares for a large number of women wanting natural births, is my business to know what is in them. I definitely have my favorites and regularly refer my patients to one book or another, depending on their needs. However, as I worked to build support for naturally laboring moms within my delivering hospitals and tried to offer my patients better options and techniques for working through their unmedicated births, I found the supply of books and information about natural birth lacking. Here are some of the main challenges I discovered:
|
AuthorDr. Michelle Aristizabal is a board-certified General Obstetrician and Gynecologist in Montclair, NJ. She is the author of Natural Labor and Birth: An evidenced-based review of the natural birth plan and runs a busy, private practice, with a special focus on supporting women who desire low-intervention, un-medicated births. Archives
February 2022
Categories |




 RSS Feed
RSS Feed